
Retinal vein occlusion is when one of the tiny retinal veins becomes blocked by a blood clot. It usually leads to a painless decrease in vision in one eye. Risk factors include high blood pressure, high cholesterol levels, diabetes, smoking and glaucoma (raised pressure in the eye). Treatment includes treating any possible risk factors and also treating any complications.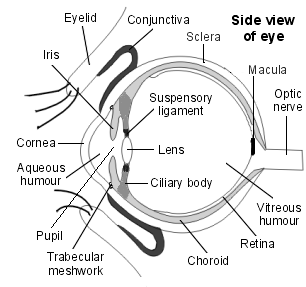
Some anatomy of the eye
When you look at an object, light from the object passes through the cornea of your eye, then the lens, and then it hits the retina at the back of your eye. The cornea and the lens both help to focus the light on to your retina. Nerve messages pass from the seeing cells (rods and cones) in your retina, down nerve fibres in your optic nerve to your brain. The messages are interpreted by your brain, which enables you to see. If the retina is damaged, a clear picture cannot be produced.
The macula is a small but vital area of the retina at the back of your eye. It is about 5mm in diameter. The very centre of the macula is called the fovea. The macula is the part of the retina that is the most densely packed with seeing cells. The macula is responsible for your central (focussed) vision. The rest of the retina is responsible for your peripheral (side) vision. The inner layers of the retina get their blood supply from the retinal arteries and retinal veins which run within the retina itself. The retinal arteries help to take oxygen and nutrients to the retina. The retinal veins drain blood away from the retina and back towards the heart.
What is retinal vein occlusion and what causes it?
Retinal vein occlusion is when one of the tiny retinal veins becomes blocked by a blood clot. This means that blood cannot drain away from the retina as easily and there is a backlog of blood in the blood vessels of the retina. This can lead to a build-up of pressure in the blood vessels. As a result, fluid and blood start to leak from the blood vessels, which can damage and cause swelling of the retina, affecting your eyesight. There are two main types of retinal vein occlusion:
- Branch retinal vein occlusion - the blockage occurs somewhere along the course of one of the four retinal veins. (One retinal vein drains each quarter of the eye.)
- Central retinal vein occlusion - the blockage occurs in the main vein formed by the four retinal veins coming together. Branch retinal vein occlusion is two to three times more common than central retinal vein occlusion.
How common is retinal vein occlusion and who gets it?
Retinal vein occlusion is a fairly common cause of loss of vision. It is most common in people over the age of 60 and it seems to affect both sexes equally.
What causes retinal vein occlusion?
The exact reason why a blood clot may form in one of the retinal veins is not clear. However, there are some things that are thought to increase your risk of developing retinal vein occlusion. They include the following.
Having risk factors for cardiovascular disease
Cardiovascular diseases are diseases of the heart or blood vessels caused by atheroma. Patches of atheroma are like small fatty lumps that develop within the inside lining of arteries (blood vessels). Atheroma is also known as atherosclerosis or hardening of the arteries. A patch of atheroma makes an artery narrower. Your risk of developing retinal vein occlusion seems to be increased if you have risk factors for cardiovascular disease. These include:
- High blood pressure - between 6 and 7 in every 10 people with retinal vein occlusion have high blood pressure. If high blood pressure is not well-controlled, it can also increase your risk of having another episode of retinal vein occlusion (either in the same eye or the other eye).
- High cholesterol
- Diabetes
- Smoking
The retinal arteries and veins run very closely together. If someone has narrowing of their retinal artery blood vessels due to atherosclerosis, this can make the artery blood vessels very rigid. It is thought that a rigid artery may then press on a close-by vein and disturb the blood flow in the vein. This turbulent blood flow means that a clot is more likely to form in the vein, leading to retinal vein occlusion.
Other possible risk factors
If you have a blood clotting problem such as antiphospholipid antibody syndrome, this can increase your risk of developing retinal vein occlusion. Having glaucoma also seems to be a risk factor.
What are the possible complications of retinal vein occlusion?
There are some complications that can develop if you have retinal vein occlusion, which may lead to worsening visual loss. The complications can include:
Macular oedema. This is swelling of the macula at the centre of the retina and is the main reason why someone with retinal vein occlusion may develop permanent visual problems.
Neovascularisation. This is abnormal new blood vessel formation at the back of the eye. About one third of people with retinal vein occlusion develop this problem. If abnormal new blood vessels form, this can sometimes lead to increased pressure within the eye and to glaucoma. Also, the new blood vessels are of a poor quality and can sometimes bleed. Another complication is that the new blood vessels can increase the risk that the retina becomes detached.
What are the symptoms of retinal vein occlusion?
If you have retinal vein occlusion, you will usually notice a decrease in vision in one eye. Some people describe having a blind spot in one eye. The condition is mostly painless unless there are complications such as secondary glaucoma caused by new blood vessels interfering with the drainage of fluid from inside the eye. Depending on the severity and also the degree of involvement of the macula, retinal vein occlusions may cause only mild visual loss in some cases or very profound visual loss in others. Some people who only have a small blockage of a branch retinal vein may not have any symptoms.
How is retinal vein occlusion diagnosed?
Retinal vein occlusion is usually diagnosed after an eye specialist examines the back of your eye, using an ophthalmoscope (a hand-held instrument with a light and magnifier). They may also use a larger special light and magnifier (which you sit at and put your chin on) called a slit lamp. The retina at the back of your eye has a typical appearance in retinal vein occlusion. Depending on the appearance of your retina, the specialist will usually be able to tell if you have a central retinal vein occlusion or a branch retinal vein occlusion. Various other tests may be suggested including measurement of your visual acuity (how well you can see) and your visual fields (to look at how good your side vision is). Some blood tests may also be suggested - for example, to check your blood sugar and cholesterol levels. Your blood pressure may also be checked. Your specialist may advise some other tests or examinations to help to see how much damage has occurred to your retina. They are usually done after some weeks and can help to plan which treatment may be best for you. The tests may include:
- Special photographs of your retina.
- Fluorescein angiography. A dye is injected (usually into your arm). The dye will then pass to and move through the blood vessels at the back of your eye and photographs can be taken with a camera to look at the blood flow to your retina.
- Optical coherence tomography. This is a special type of test that can measure the amount of macular oedema that you may have.
What is the treatment for retinal vein occlusion?
Currently, there is no treatment that can reverse the blocked vein. The aims of treatment are to detect and treat any underlying risk factors for the condition and also to detect and treat any complications where possible.
Treatment of any underlying risk factors
For example, this includes:
- Treatment of high blood pressure. (A separate leaflet called 'High Blood Pressure (Hypertension)' gives further details.)
- Treatment of raised cholesterol levels. (A separate leaflet called 'Cholesterol' gives further details.)
- Good control of diabetes. (A separate leaflet called 'Diabetes Type 2' gives further details.)
- Giving up smoking if you are a smoker. (A separate leaflet called 'Smoking - Tips to Help you Stop' gives further details.)
- Treatment for blood clotting disorders or rare blood problems.
- Diagnosis and treatment of glaucoma.
Treatment of any complications
Someone with retinal vein occlusion needs close follow-up so that any complications can be picked up early and treated where possible. Laser treatment can be used to help treat both macular oedema and abnormal blood vessel development. A different kind of laser can be used where the vein occlusion causes neovascularisation leading to glaucoma. There is a lot of research looking into the best way to treat retinal vein occlusion. Various new treatments are being researched. For example, steroid injections into the eye (the damaged retina becomes inflamed and steroids may help to reduce inflammation). A chemical called vascular endothelial growth factor (VEGF) is released by the damaged retina. Injections of a drug which blocks this has been used with some success (eg Avastin, Lucentis)
What is the prognosis (outlook)?
Following a retinal vein occlusion you are likely to be left with some visual loss. The extent of the visual loss can vary greatly, depending on the severity and exact site of the vein occlusion. Early diagnosis and treatment of retinal vein occlusion and any complications may make a difference to the eventual level of visual loss. However, severe vein occlusions can cause permanent visual loss, even if treated very early. Retinal vein occlusion will recur in about 1 in 6 people (either in the same eye or in the other eye) over the five years following on from it.
Can retinal vein occlusion be prevented?
The same things that can help to reduce your risk of cardiovascular disease may also possibly reduce your risk of retinal vein occlusion. For example:
- Treating high blood pressure if you have high blood pressure.
- Good control of diabetes if you have diabetes.
- Stopping smoking if you are a smoker.
- Reducing high cholesterol levels if they are raised.
- Aiming to be physically active and do regular exercise, if possible.
- Losing weight if you are overweight.